Otoscopy Learning Module
Basics of hearing
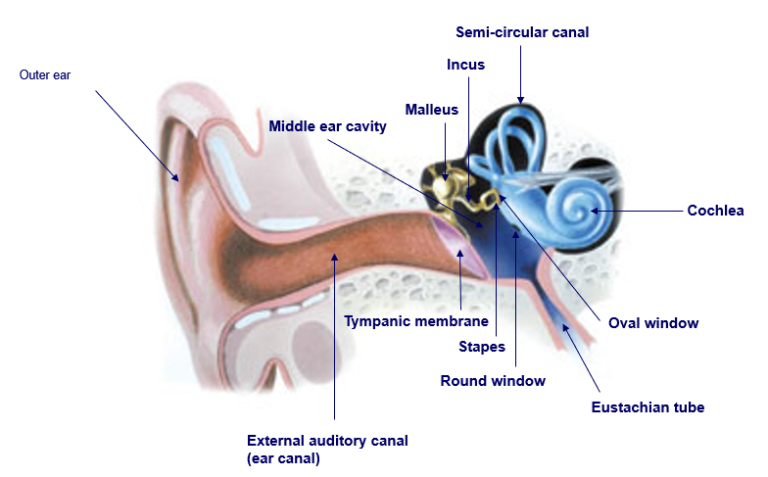
- 1. The sound waves are funnelled by the outer ear through the ear canal into the middle ear. The eardrum vibrates from the incoming sound waves and these vibrations get amplified by three tiny bones in the middle ear (malleus, incus and stapes) before getting transmitted to the cochlea (snail-like structure filled with fluid) in the inner ear. An elastic partition known as the basilar membrane runs from the beginning to the end of the cochlea. The vibrations cause the fluid to ripple and a wave forms along the basilar membrane.
- 2. Sensory cells sitting on top of the membrane called hair cells move with the wave - higher-pitched sound are detected by those cells near the wide end of the cochlea whereas lower-pitched sounds are detected nearer the centre. This up and down movement of the hair cells causes the stereocilia (microscopic hair-like projections that sit on top of the hair cells) to bump against an overlying membrane and deflect. Pore-like channels are found at the top of the stereocilia.
- 3. When they get deflected, those channels open up and chemicals rush into the cells, generating an electrical signal.
- 4. This electrical signal (an action potential) travels along the auditory nerve to the brain which processes it and turns it into a sound as we know it.
Otoscopy
Importance of training
Several studies have found that otolaryngology training had a significant impact on the success rate of diagnosis when an otoscope was used by a non-specialist (Damery et al., 2018; Oyewumiet al., 2016). Studies on the use of video-otoscopy by untrained healthcare workers or by the general population yielded similar results (Shah et al., 2018, Demantet al., 2019). The importance of otolaryngology training should therefore be emphasized to the non-OTO-HNS clientele making use of an otoscope, whether it be handheld or fitted to a device. This is particularly true with the rapid advance of telemedicine.


Video- or remote otoscopy
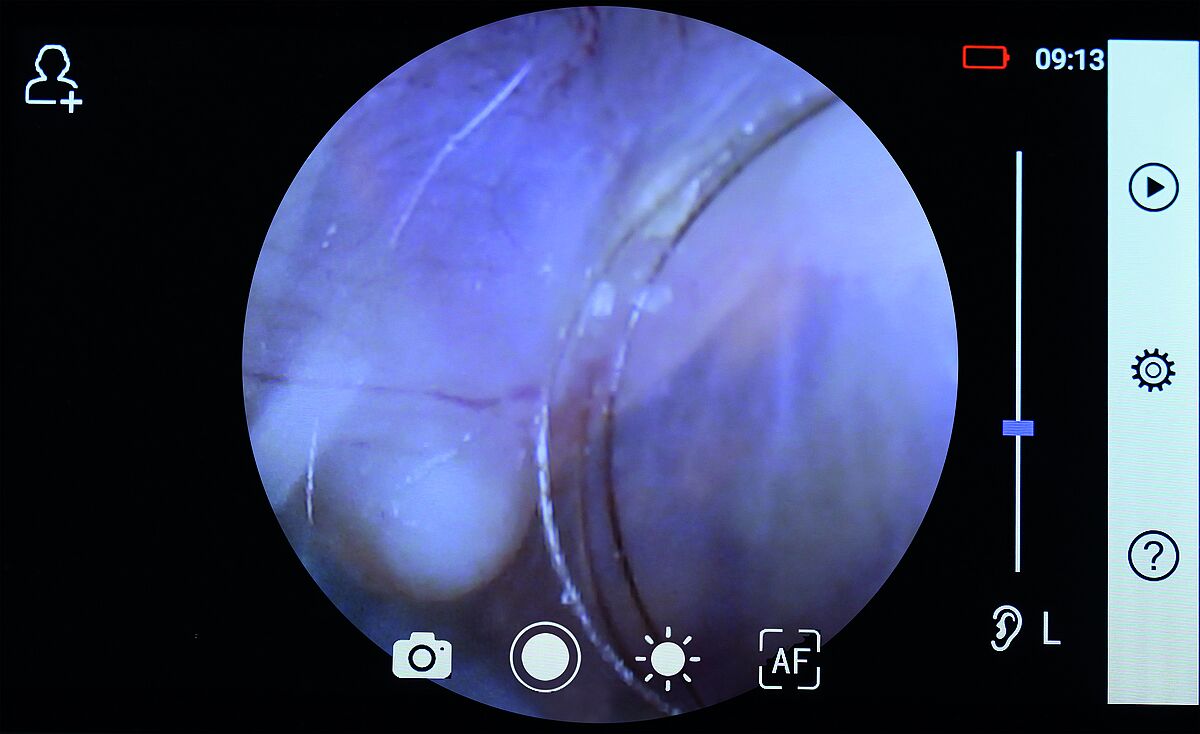
Digital, portable and multifunctional medical camera system are available and offer the possibility of fitting an otoscope lens. Thanks to their ease of use and portability, an examiner in a remote location can capture images that will be sent to a physician for evaluation, or even be evaluated live via telemedicine, thereby making specialist healthcare more accessible. Several research studies have already been conducted and support the benefit of video-otoscopy, both in a synchronous and asynchronous manner. A study by Lundberg et al. (International Journal of Pediatric Otorhinolaryngology, 2017) which aimed to compare otoscopy performed by a general practitioner with video-otoscopy performed remotely and assessed asynchronously concluded the following:
“Video-otoscopy performed by a health care facilitator and assessed asynchronously by a general practitioner had similar or better accuracy compared to face-to-face otoscopy performed by a general practitioner.”
Left: Riester’s RCS-100 equipped with the otoscope lens and an image it captured of an eardrum. Riester’s RCS-100 allows for both imaging and videoing of the eardrum and is suitable for synchronous or asynchronous diagnosis.
Key take-aways:
- Video-otoscopy improves the diagnosis of GPs when examining pathological eardrums.
- Video-otoscopy performed by non-medical staff and reviewed asynchronously by a GP showed equivalent or better accuracy when compared to a conventional otoscopic examination by a GP.
- Video-otoscopy performed by non-medical staff with little to no prior medical experience in rural Kenya and reviewed asynchronously by an otolaryngologist successfully identified several pathologies in children: complete cerumen impaction, effusion, retraction, perforation, otitis media, CSOM and fungal otitis media.

Otoscope
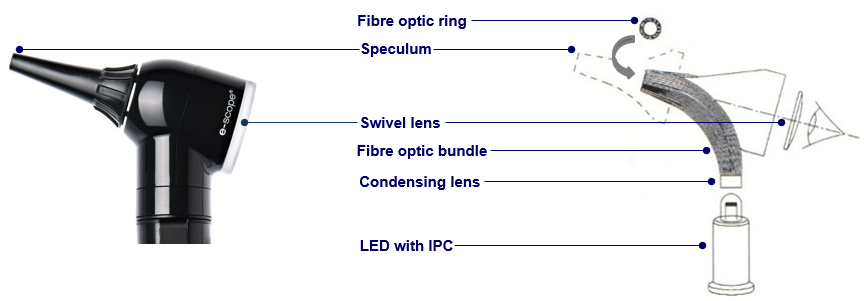
An otoscope is an instrument that allows a user to look into the ear. The cylindrical handle contains the batteries and the head is comprised of two parts: a light source in a conical viewer at one end to insert into the ear and a low-power magnifying lens at the other end to enlarge the viewing area. Most otoscopes allow instrumentation either by making the lens removable or by using an open head system such as Riester’s operation lens. Riester’s operation lens is designed for the illumination and examination of the auditory canal and for insertion of external instruments into the auditory canal. Models that allow adjustable focusing are particularly useful for examiners who are long-sighted. Where increased magnification is necessary, a macro-otoscope can be used (e.g. Riester’s EliteVue fibre optic macro-otoscope). It is simply a variant on the standard otoscope which boosts the magnification to over 5x as opposed to the standard 3x.

Otoscope: handle and speculum
Pneumatic otoscope
An otoscope compatible with pneumatic otoscopy integrates a port to house an insufflation bulb that applies positive and negative air pressure to the eardrum. It is sometimes referred to as pneumatoscope when assembled. When a speculum is simultaneously attached to the head and fitted snugly into the patient’s ear canal, an air-tight chamber is generated. The behaviour and mobility of the tympanic membrane are observed through the lens as the bulb is being pressed. A healthy membrane moves in response to the pressure generated. Pneumatic otoscopy can help with the diagnosis of pathologic eardrums because a perforation, tympanosclerosis or the presence of fluid in the middle ear (key element of the diagnosis of otitis media with effusion) can render the tympanic membrane immobile.
Tip: Depending on the size of the ear canal, it may be difficult to create a seal using readily available specula. This difficulty can be alleviated by using a piece of medical adhesive tape (1/2 inch wide, length approx. 4 inch but may be shorter or longer depending on thickness needed to create seal), placed about 1/4 inch proximal to the tip of the speculum and wrapped around it to create a thick and soft bevel.

What to choose?
Light transmission

Two ratings are typically used when describing a light source: the colour-rendering index and the Kelvin colour temperature scale.
In short, the higher the Kelvin rating, the whiter the light and the closer to 100 the CRI rating, the higher the quality of its colour compared to the light spectrum we can see thanks to the sun (natural daylight).
Light source
Otoscopes come with either a filament bulb (halogen, xenon) or a LED bulb.
-
Lighting: filament vs LED
An accurate pigmentation is made possible by the use of LED light due to its natural temperature colour. LED also provides more consistent light throughout the whole area being viewed than halogen. While xenon has long been favoured for high-end medical lighting applications due to its bright, white light, LED bulbs can now produce a similar level of bright, white light. -
Lifetime: filament vs LED
An LED bulb can last between 50,000-100,000 hours, more than 10x longer than an average filament bulb. This is 6-12 years of continuous use before needing replacement. -
Heat release: filament vs LED
Filament bulbs produce a lot of heat (risk of burns or fire). LED bulbs are cool to the touch which makes them safer. -
Cost: filament vs LED
Filament bulbs are cheaper to replace than LED bulbs. LED bulbs have a higher cost upfront but last exponentially longer and require less maintenance, making them a cheaper alternative over the long run.
Damery, E. Lescanne, K. Reffet, C. Aussedat, D. Bakhos, Interest of video-otoscopy for the general practitioner, European Annals of Otorhinolaryngology, Head and Neck Diseases, Volume 136, Issue 1, 2019, Pages 13-17, ISSN 1879-7296, https://doi.org/10.1016/j.anorl.2018.10.016.
How Do We Hear? | NIDCD (nih.gov)
Kristen L. Yancey, Loyce J. Cheromei, Jackie Muhando, Jim Reppart, James L. Netterville, Asitha D.L. Jayawardena, Pediatric hearing screening in low-resource settings: Incorporation of video-otoscopy and an electronic medical record, International Journal of Pediatric Otorhinolaryngology, Volume 126,2019, 109633, ISSN 0165-5876, https://doi.org/10.1016/j.ijporl.2019.109633.
Malene Nøhr Demant, Ramon Gordon Jensen, Mahmood F. Bhutta, Gunnar Hellmund Laier, Jørgen Lous, Preben Homøe, Smartphone otoscopy by non-specialist health workers in rural Greenland: A cross-sectional study, International Journal of Pediatric Otorhinolaryngology, Volume 126, 2019, 109628, ISSN 0165-5876, https://doi.org/10.1016/j.ijporl.2019.109628.
Manan Udayan Shah, Maheep Sohal, Tulio A. Valdez, Christopher R. Grindle, iPhone otoscopes: Currently available, but reliable for tele-otoscopy in the hands of parents?, International Journal of Pediatric Otorhinolaryngology, Volume 106, 2018,Pages 59-63, ISSN 0165-5876, https://doi.org/10.1016/j.ijporl.2018.01.003.
Modupe Oyewumi, Michael G. Brandt, Brian Carrillo, Adelle Atkinson, Karl Iglar, Vito Forte, Paolo Campisi, Objective Evaluation of Otoscopy Skills Among Family and Community Medicine, Pediatric, and Otolaryngology Residents, Journal of Surgical Education, Volume 73, Issue 1,2016, Pages 129-135, ISSN 1931-7204, https://doi.org/10.1016/j.jsurg.2015.07.011.
Pneumatic Otoscope Examination: Overview, Indications, Contraindications (medscape.com)
Thorbjörn Lundberg, Leigh Biagio de Jager, De Wet Swanepoel, Claude Laurent, Diagnostic accuracy of a general practitioner with video-otoscopy collected by a health care facilitator compared to traditional otoscopy, International Journal of Pediatric Otorhinolaryngology, Volume 99,2017, Pages 49-53, ISSN 0165-5876, https://doi.org/10.1016/j.ijporl.2017.04.045.