
Contact thermometers require physical contact to operate. A heat sensor is located inside the probe; when in contact with a warmer surface, conduction takes place and the sensor’s temperature rises to that of the warmer surface. There are different types of contact thermometers depending on the type of sensor used: thermocouple, resistance temperature detector (RTD) or thermistor. Thermocouple sensors are cheap and offer a wide temperature range but lack the high level of accuracy needed in healthcare services. Both RTDs and thermistors are found in medical devices and instruments with RTDs being among the most precise temperature sensors available, with measurement uncertainties of ±0.1°C (±0.18°F) or better.
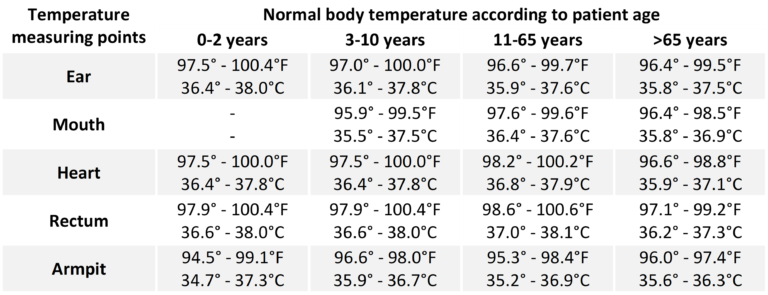
Contact thermometers can be used on the forehead, mouth, armpit or rectum. Accuracy of readings vary between age groups: the gold standard in infants (up to age 3) is rectal measurement but in older age groups, oral measurements generally provide enough accuracy as long as the mouth is kept shut. Axillary (armpit) measurements are the least accurate but may be used in non-acute and low-risk situations where a high level of accuracy is not necessary as they may be better tolerated. Rectal measurements are the most accurate regardless of the age group and should be preferred in acute and high-risk situations.
Because contact thermometers come in contact with the patient, probe covers or proper disinfection are necessary to avoid cross-contamination.
Note: while the tympanic thermometer does come in contact with the ear canal, it does not rely on a heat exchange with a heat sensor (requiring direct contact) to record temperature but rather on the measurement of infrared emissions (which can be done at a distance from a surface). For that reason, it is classified as a non-contact thermometer.

ASTM E1965-98 defines non-contact thermometers, also known as infrared (IR) thermometers, as optoelectronic instruments adapted for non-contact measurement of temperature of a subject by utilizing infrared radiation exchange between the subject and the sensor. They allow for quick readings with the possibility of avoiding direct contact and in some cases, close proximity. ASTM requires an IR thermometer for measuring skin temperature to be accurate to within ± 0.3°C (±0.54°F). For ear canal temperature, the requirement is tighter with ± 0.2°C (±0.36°F). IR thermometers used to measure human body temperature should be approved for clinical use and should offer an adjusted mode which compensates between skin temperature and body core temperature and should allow for calibration with an IR calibrator tool.
Working principle
Every form of matter with a temperature greater than absolute zero (0 K) emits infrared radiation relative to its temperature. This phenomenon is known as characteristic radiation. Different surfaces have different abilities to emit energy by radiation – in other words, they have a different emissivity. By knowing the emissivity of a surface and how much infrared energy it emits, its temperature can usually be determined. Emitted, reflected and transmitted thermal energy from the target is collected onto a lens that pass it on to a detector: the thermopile. A thermopile consists of several thermocouples connected in series and sometimes in parallel; together they convert the thermal energy from the radiation to an electrical signal. Electronic components act as the brain of the thermometer to process the signal to corelate it to the temperature that will ultimately be shown on the display.
Note: Only surface temperatures can be measured by infrared. Environmental conditions involving smoke, dust or steam reduce accuracy.
